No audio available for this content.

Trends Discerned in the National Cancer Institute’s Geospatial Databases Carry the Fight Forward
Location matters in cancer, as in many other things. The National Cancer Institute (NCI) recognized this fact more than 40 years ago, and its researchers have been investigating striking geographic differences in many cancers ever since. Most studies have found that these differences were due to lifestyle differences, such as levels of smoking and diet, although research into possible environmental causes are hampered by a lack of exposure data during the relevant period, 20–30 years prior to diagnosis.
Geospatial tools serve NCI in a variety of applications, including:
- the identification and display of the geographic patterns of cancer incidence and mortality rates in the U.S. and their change over time,
- the creation of complex databases for the study of cancer screening, diagnosis, and survival at the community level,
- environmental exposure assessment through satellite imagery,
- spatial statistical models to estimate cancer incidence, prevalence, and survival for every U.S. state,
- communication of local cancer information to the public and public health professionals through interactive web-based tools,
- the identification of health disparities at the local level through the comparison of cancer outcomes across demographic subgroups, and
- development of new methods of displaying geospatial data for clear communication to the public and for examination of complex multivariate data by researchers.
Division of Cancer Control and Population Sciences
The Epidemiology and Genomics Research Program (EGRP) and the Surveillance Research Program (SRP) support grant research to use GIS in cancer research and the development of methodologies to accomplish this research. EGRP also funded the development and maintenance of a geographic information system for breast-cancer studies on Long Island (LI GIS). The LI GIS is available to researchers and can be used to study other types of cancer and conditions as well.
Surveillance Research Program
The Statistical Methodology and Applications Branch (SMAB) contributes to GIS research by developing statistical methods for the analysis, display, and web-based communication of geo-referenced cancer data.
The Surveillance Systems Branch (SSB) oversees the Surveillance, Epidemiology, and End Results (SEER) program, an integrated, comprehensive, multiple population-based reporting system of cancer registries covering 26% of the U.S. population. Cancer incidence information is provided at the state, county, and census-tract level. Investigators in SEER’s Rapid Response Surveillance Studies (RRSS) are exploring and applying GIS technology in several areas.
Division of Cancer Epidemiology and Genetics
The Epidemiology and Biostatistics Program (EBP) has a long history of publishing the NCI cancer atlases.
The Occupational and Environmental Epidemiology Branch (OEEB) has an active research program in using satellite imagery to estimate the potential exposure to cancer-causing environmental agents by individuals living in agricultural areas.
As to the finer granularity customarily seen in GIS databases by professionals using them in mapping, natural resource and asset management, utilities, and other sectors, researcher Linda Pickle of Pennsyslvania State University and StatNet Consulting comments:
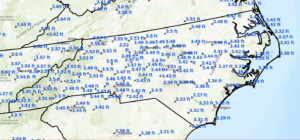
“The SEER program at NCI does get the census-tract identification from the registries, but you have to get permission to use it. Mortality is only reported to NCHS at the county level. Therefore, all nationwide maps of cancer rates (incidence or mortality) must be at the geographic level available for all states, that is, county. Each state has the option to present its own data at smaller levels.
“Figure 2 gives an example of sub-county maps published by California Cancer registries. California is densely populated in many counties, and so the state has defined aggregations of census tracts for their maps. Some of California is in the SEER program; other parts have registries funded by the Centers for Disease Control (CDC).”

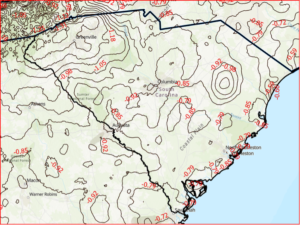
“Another state example: the Kentucky SEER registry has developed a useful online tool to explore Kentucky cancer patterns,” Pickle said. “See Figure 3. This design has been used by CDC for an online U.S. cancer atlas and by other states.”

 FURTHER READING
FURTHER READING

Visualizing Data Patterns with Micromaps By Daniel B. Carr and Lindia Williams Pickle
Available on Amazon and Barnes & Noble.
Read more about GPS World’s cancer research special coverage from Editor Alan Cameron.
Patterns of Childhood Cancer
Cancer surveillance — an assessment of the number and type of cancer cases that occur in an area and in a specified population — provides critically important information needed for determining geographic variations in cancer rates and for planning cancer control intervention programs.
By Li Zhu, Linda W. Pickle, Zhaohui Zou, and James Cucinelli
This article is about projecting from the data that were available from surveillance/data-collection efforts to get estimates of the number of new cancer cases that would occur in the upcoming calendar year. That is, we used data from up to four years previous (because of the time it takes to find cases, process data, and so on) to get a current estimate of the number of cases.
We developed the statistical model to do this in 2006, then validated it, modifying the temporal projection method a few years ago. This method was then adopted by the American Cancer Society to produce the numbers of new cases published in their annual Cancer Facts & Figures reports, the most cited cancer reference in the world.
Since the models did not break out childhood cancers, we repeated the modeling process to do that, resulting in the paper cited here.
The method requires first a spatiotemporal prediction across the extensive years of data, since not all cancer registries have data for every year, and secondly a four-year temporal projection from the most current data point to the current calendar year. Here we use this same process applied only to childhood cancer data.
The generalized linear mixed effects model is applied to observed childhood cancer case counts reported to the North American Association of Central Cancer Registries over 1995– 2006 to predict case counts and incidence rates for every U.S. state and the U.S. total (for patients aged 0 to 19 and for major cancers among childhood). Covariates included in the model are measures of income, education, housing, urban/rural status, health insurance coverage, smoking, obesity, and cancer screening. Temporal trends and spatial distribution patterns are compared among childhood cancers for males and females.
Results. A total of 15,168 new cancer cases was projected for the 0–19 age group, with 10,032 childhood cancer cases younger than age 15, and 5,136 cases in the 15–19 age group, in the United States for 2010. There are more male cancer cases than female cases in all three age groups for most cancer sites. The order for the most common malignancies diagnosed in children differs by age group and sex. The study also identifies differences in the geograhic patterns at a small geographic area level by gender, and temporal trends by gender and subsites of childhood cancer incidence.
Conclusions. The resulting set of predictions provides annual estimates for states that did not provide data at all, and projections ahead in time to the current calendar year for every U.S. state and the United States in total. These projections fill in the data gaps for recent years of diagnosis and state registries to provide complete count and rate estimates for childhood cancers for all states, regions, and the U.S. in total for the current calendar year.
(The full article, “Trends and patterns of childhood cancer incidence in the United States, 1995–2010,” appears in Statistics and Its Interface, Volume 7 (2014), pp. 121-134.)


Urban Sprawl, Obesity, and Cancer Mortality
Cross-Sectional Analysis and Methodological Challenges
By David Berrigan, Zaria Tatalovich, Linda W. Pickle, Reid Ewing, and Rachel Ballard-Barbash
Urban sprawl has the potential to influence cancer mortality via direct and indirect effects on obesity, access to health services, physical activity, transportation choices, and other correlates of sprawl and urbanization.
Methods. This paper presents a cross-sectional analysis of associations between urban sprawl and cancer mortality in urban and suburban counties of the United States.
A major focus of our analyses was to adequately account for spatial heterogeneity in mortality. Therefore, we fit a series of regression models, stratified by gender, successively testing for the presence of spatial heterogeneity. Our resulting models included county-level variables related to race, smoking, obesity, access to health services, insurance status, socioeconomic position, and broad geographic region, as well as a measure of urban sprawl and several interactions.
Results. Total cancer mortality rates were higher in less sprawling areas and contrary to our initial hypothesis; this was also true of obesity-related cancers in six of seven U.S. regions (census divisions) where there were statistically significant associations between the sprawl index and mortality. We also found significant interactions between region and urban sprawl for total and obesity-related cancer mortality in both sexes.
Conclusions. Despite higher levels of obesity in more sprawling counties in the U.S., mortality from obesity-related cancer was not greater in such counties. Identification of disparities in cancer mortality within and between geographic regions is an ongoing public health challenge and an opportunity for further analytical work identifying potential causes of these disparities. Future analyses of urban sprawl and health outcomes should consider exploring regional and international variation in associations between sprawl and health.
“Urban sprawl, obesity, and cancer mortality in the U.S.: cross-sectional analysis and methodological challenges,” in International Journal of Health Geographics, January 2014.)
GPS-Measured Physical Activity in Non-Small-Cell Lung Cancer
By C.L. Granger, L. Denehy, C.F. McDonald, L. Irving, R.A. Clark
Physical activity (PA) is increasingly recognized as an important outcome in non-small-cell lung cancer (NSCLC). We investigated PA using GPS, tracking individuals with NSCLC and similar-aged healthy individuals.
Methods. Fifty individuals with NSCLC and 35 similar-aged healthy individuals without cancer were included. Primary measures were triaxial accelerometery (steps/day) and GPS tracking (outdoor PA behavior). Secondary measures were questionnaires assessing depression, motivation to exercise, and environmental barriers to PA.
Results. Individuals with NSCLC engaged in significantly less PA than similar-aged healthy individuals and had higher levels of depression and lower motivation to exercise. Daily outdoor walking time and distance traveled away from home were not different between groups. Individuals with NSCLC spent less time outdoors in their local neighborhood area. A greater number of steps per day was seen in patients who were less depressed or had better access to nonresidential destinations such as shopping centers.
(The full article, “Physical Activity Measured Using Global Positioning System Tracking in Non-Small Cell Lung Cancer: An Observational Study,” appears in Integrative Cancer Therapies, July 2014.)










John
“GIS Builds Awareness, Improves Treatment, Aids Prevention” There’s a word missing in your title: cancer.